Hypodontia
Hypodontia means that there are fewer than the normal complement of teeth in the dentition. It may be an isolated single tooth missing with no known etiology or it could be associated with a syndrome due to an event occurring before tooth germ formation.
|
|

|
The incidence of hypodontia is <1% in the primary dentition incidence and is approximately 2.5-3.5% in the secondary dentition.
The secondary teeth most frequently missing are the
third molars
second premolars
maxillary lateral incisors
|
|
The image above is an example of an abnormality of numbers (congenitally missing permanent maxillary left lateral incisor) and an abnormality of shape. The permanent maxillary right lateral incisor is a peg lateral incisor (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba)
|
|
|
|
This is an example of a retained primary molar (primary mandibular right second molar) and a single congenitally missing tooth (permanent mandibular right second premolar).
|
|

|
The image on the left is another example of an abnormality of numbers (congenitally missing permanent maxillary right lateral incisor) and an abnormality of shape. The permanent maxillary left lateral incisor is a peg lateral incisor (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
.
|
|

|
|
The panoramic radiograph above illustrates a case of a congenitally missing permanent maxillary right lateral incisor. The permanent mandibular right third molar had been previously extracted (courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|

|
The bitewing radiograph on the left is of the patient's posterior right and illustrates the posterior teeth in quadrants 1 and 4. The primary maxillary right second molar is retained and the permanent maxillary right second premolar is congenitally missing (courtesy of Dr. BM Cleghorn, Dalhousie University).
.
|
|

|
|
The panoramic radiograph above illustrates a congenitally missing permanent maxillary right lateral incisor (arrow labeled 1.). The arrow labeled 2. is an example of an abnormality in shape as the permanent maxillary left lateral incisor is a peg lateral (courtesy of Dr. BM Cleghorn, Dalhousie University).
.
|
|

|
|
This panoramic radiograph is suggestive of a patient with ectodermal dysplasia. The clinical findings were inconclusive and confirmation of the diagnosis is awaiting genetic testing. Congenitally missing teeth include the permanent maxillary right second premolar, permanent mandibular left first and second premolars and the permanent mandibular right second premolar. Ankylosed primary teeth are present as well as an anomalous permanent maxillary left first premolar. The full case report labeled Case RT is included later in this unit (courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|

|
The periapical radiograph on the left illustrates a single congenitally missing tooth. The arrow points to the congenitally missing permanent mandibular left second premolar. Above the arrow is the retained primary mandibular left second molar with partially resorbed roots (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|

|
The illustration on the left is an example of induced anodontia. True anodontia is rare. This patient has been rendered edentulous as a result of caries or periodontal disease (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|

|
The patient on the left only has four permanent canines remaining. Each of these teeth has been restored with full crowns. This condition is described as partial anodontia (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
Oligodontia
Oligodontia is considered a subset of hypodontia and is due to an event that occurs before tooth germ formation. 6 or more teeth are missing. Oligodontia is usually associated with a syndrome.
|
|

|
|
This panoramic radiograph is an example of oligodontia (6 missing teeth). Also present is a peg lateral incisor.
1. congenitally missing permanent maxillary right second premolar.
2. congenitally missing permanent maxillary right lateral incisor.
3. peg lateral incisor.
4. congenitally missing permanent maxillary left first premolar.
5. congenitally missing permanent maxillary left second premolar.
6. congenitally missing permanent mandibular left second premolar.
7. congenitally missing permanent mandibular left first premolar.
8. congenitally missing permanent mandibular right second premolar.
(courtesy of Dr. BM Cleghorn, Dalhousie University)
|
|

|
The image on the left is an example of ectodermal dysplasia. The only teeth present are anomalous permanent mandibular canines. Ectodermal dysplasia is comprised of a group of inherited conditions that affects ectodermal structures (such as skin, teeth, hair, salivary and sweat glands). This condition can result in multiple missing teeth (hypodontia or oligodontia). This is an example of oligodontia. More than six teeth are missing and the remaining ones are abnormally formed. Therefore, in addition, this is also an example of an abnormality of shape (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
Hyperdontia
|
|
|

|
|
The panoramic radiograph above is an example of a patient with cleidocranial dysplasia. This is an autosomal dominant genetic disorder that affects the face, the skull and the clavicles. The ossification of the clavicles, cranium and other long bones is defective. The clavicular defects can result in the patient being able to touch their shoulders. The intraoral features include multiple unerupted supernumerary teeth and delayed eruption of the permanent teeth (courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|
|

|
The occlusal view of the mandibular arch pictured on the left illustrates a slightly crowded arch. Close examination reveals a supernumerary mandibular central incisor. This is not a common anomaly and illustrates the importance of careful identification and charting in dentistry (courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|

|
The periapical radiograph of the 4th quadrant to the left illustrates a supernumerary mandibular right premolar.
1. permanent mandibular right second premolar.
2. supernumerary mandibular right second premolar.
3. permanent mandibular right first premolar.
(courtesy of Dr. BM Cleghorn, Dalhousie University)
|
|

|
Many mesiodens remain unerupted. This is an example of a fully erupted mesiodens lingual to the permanent maxillary left central incisor (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
.
|
The term microdontia means 'small teeth'. True microdontia can be differentiated from relative microdontia associated with macrognathia (teeth of normal size in a larger than normal jaw) by referring to a table of average values (such as Linek's Tooth Carving Manual). Microdontia may occur as a single entity in a normal dentition or it can be associated with syndromes such as Down syndrome and pituitary dwarfism.
The radiograph on the left is an example of a microdont secondary (permanent) canine (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). The average length of a permanent mandibular canine is 27.5mm (Goodacre, CJ, 2003) while the average length of the mandibular lateral incisor is 23.4mm. The lateral incisor is normal in length.
The clinical photo on the left shows microdont secondary (permanent) mandibular central incisors (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). Both mandibular central incisors have conical-shaped crowns.
Fusion
Fusion is defined as the union of enamel and dentin between two teeth. A differential diagnosis must differentiate fusion from concrescence and gemination. The incidence of fusion is approximately 0.5 % in the primary (deciduous) dentition and 0.1% in the secondary (permanent) dentition. The tooth presents as a macrodont with a separate root canal system (compare to gemination). The total number of teeth in the dentition is reduced by one.
Teeth Most Commonly Associated with Fusion
Maxillary central and lateral incisors
 The clinical photo on the left is an example of fusion between a permanent maxillary left central incisor and a supernumerary tooth. The permanent maxillary right and left lateral incisors are unerupted. The primary maxillary left lateral incisor and canine are present in this photo (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). The clinical photo on the left is an example of fusion between a permanent maxillary left central incisor and a supernumerary tooth. The permanent maxillary right and left lateral incisors are unerupted. The primary maxillary left lateral incisor and canine are present in this photo (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|

Fusion of the permanent maxillary right central and lateral incisors (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|
 The clinical photo on the left is an example of bilateral fusion of primary mandibular incisors. The primary mandibular right central and lateral incisors are fused as are the primary mandibular left central and lateral incisors (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). The clinical photo on the left is an example of bilateral fusion of primary mandibular incisors. The primary mandibular right central and lateral incisors are fused as are the primary mandibular left central and lateral incisors (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|
|
 The print of the radiograph on the left illustrates fusion between the primary mandibular left lateral incisor and the primary mandibular left canine. Two separate root canal systems are visible (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). The print of the radiograph on the left illustrates fusion between the primary mandibular left lateral incisor and the primary mandibular left canine. Two separate root canal systems are visible (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|
Dens invaginatus (dens in dente)
Oehlers classification of this condition continues to be used today (Oehlers, FAC, 1957a, Oehlers, FAC, 1957b and Oehlers, FAC, 1958). Forms include coronal (most common) and radicular type. The incidence ranges from 0.04 to 10% in all populations. "Dens in dente" is a misnomer because it means "tooth within a tooth". This is not really a tooth because it is lined by enamel only appears to be like a tooth radiographically. The severity can range from a pit to a dilated odontome. Treatment can range from restorative to extraction of the tooth.
 The clinical photo on the left is an example of dens invaginatus associated with the permanent mandibular left first and second premolars (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). The clinical photo on the left is an example of dens invaginatus associated with the permanent mandibular left first and second premolars (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|

Dens invaginatus associated with the permanent maxillary right central incisor (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|
 The clinical photo on the left illustrates dens invaginatus associated with the permanent maxillary left lateral incisor (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). The clinical photo on the left illustrates dens invaginatus associated with the permanent maxillary left lateral incisor (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|
Amelogenesis Imperfecta
This is an ectodermal disorder and therefore affects the enamel only. The incidence ranges from .01% to .14% depending on the population At least 18 subtypes (Witkop, CJ, 1988) have been identified based on clinical features, light microscopic appearance and the inheritance pattern. This defect affects both the primary and secondary dentitions. Multiple modes of inheritance including autosomal dominant and autosomal recessive are possible.
Features of amelogenesis imperfecta include openbite due to attrition, eruption may be normal or late and the dentinoenamel junction is scalloped. Affected teeth are discoloured (exogenous pigment) and may be pitted, rough or smooth enamel. Enamel is thin or mottled radiographically. Problems include aesthetics, abrasion, sensitivity and caries susceptibility. Pathogenesis is a progressive, functional defect of ameloblasts. Management may include crowns (full coverage) and possibly full mouth osteoplasty (recontouring of bone) to increase the length of the clinical crowns for retention of full veneer crowns.

Pitted form of amelogenesis imperfecta
(courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|

Snow-capped form of amelogenesis imperfecta (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|
A case study of a Type IE X-linked (dominant) smooth hypoplastic amelogenesis imperfecta (Witkop's classification) is presented to illustrate the inheritance pattern of one type of amelogenesis imperfecta. This subtype of AI (amelogenesis imperfecta) was diagnosed through the use of a pedigree and examination of all the members of the M family. The father Chris M had severe, generalized hypoplastic defects of the enamel. A pedigree illustrated that this defect was only transferred to the female children (Katrina M and Maria M). Son Marcus M had a normal dentition. The defects in the teeth of the female children were somewhat less severe than in the father but resulted in vertical banding of the enamel. A diagnosis of Type IE X-linked (dominant) smooth hypoplastic amelogenesis imperfecta was made based on a pedigree and clinical examination of all family members. The pattern of enamel defects in the family are illustrated below.
|
|

|
Chris M

Amelogenesis Imperfecta
Father Chris M as he initially presented. Maxillary teeth had been treated with metal ceramic crowns. Mandibular teeth are virtually devoid of enamel (courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|
 Occlusal view of Chris M illustrating normal tooth morphology and hypoplastic enamel Occlusal view of Chris M illustrating normal tooth morphology and hypoplastic enamel
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|

Right BW radiograph
Chris M
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|

Left BW radiograph
Chris M
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|

Right PA radiograph
Chris M
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|

Left PA radiograph
Chris M
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
Katrina M
|
|
 Pre-treatment frontal view of daughter Katrina M aged 12 years 9 months Pre-treatment frontal view of daughter Katrina M aged 12 years 9 months
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
 Maxillary left quadrant close-up of vertical banding of enamel in patient Katrina M illustrating severely hypoplastic enamel Maxillary left quadrant close-up of vertical banding of enamel in patient Katrina M illustrating severely hypoplastic enamel
|
|
|

Right BW radiograph
Katrina M
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|
|
|
 Left BW radiograph Left BW radiograph
Katrina M
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|
|
|
 Post-treatment frontal view of Katrina M Post-treatment frontal view of Katrina M
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
 Post-treatment view of maxillary arch of Katrina M with full coverage of all teeth Post-treatment view of maxillary arch of Katrina M with full coverage of all teeth
|
|
Vickie M
|
|
|
|
 Pre-treatment frontal view of Vickie M aged 5 years 4 months Pre-treatment frontal view of Vickie M aged 5 years 4 months
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
 Pre-treatment view of maxillary left quadrant of patient Vickie M Pre-treatment view of maxillary left quadrant of patient Vickie M
|
|
|
 Pre-treatment occlusal view of maxillary arch of Vickie M Pre-treatment occlusal view of maxillary arch of Vickie M
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
 Pre-treatment occlusal view of mandibular arch of Vickie M Pre-treatment occlusal view of mandibular arch of Vickie M
|
|
Marcus M
Marcus and brother Chris Jr. were unaffected by this sex-linked Type IE X-linked (dominant) smooth hypoplastic amelogenesis imperfecta.
|
|
|
|
 Frontal view of Marcus M Frontal view of Marcus M
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|
|
|
 Right BW Right BW
Marcus M
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|
|
|
 Left BW Left BW
Marcus M
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|
|
Chris Jr.
|
|
|
|
 Frontal view of Chris Jr. aged 3 years 5 months Frontal view of Chris Jr. aged 3 years 5 months
(courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|
|
Dentinogenesis imperfecta
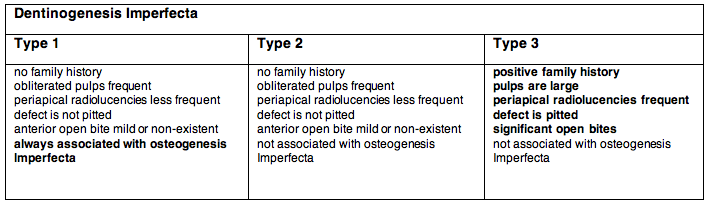
This is a mesodermal defect that affects the dentin. The condition is also called hereditary opalescent dentin and can be seen in isolation or associated with a systemic defect (osteogenesis imperfecta). Both the primary and secondary dentitions are affected. Dentinogenesis Imperfecta (DI) is a genetic disorder with an autosomal dominant mode of inheritance. The teeth are blue or brown and translucent. The incidence is approximately 1 in 8,000 in the USA. The classification system for this entity is less than perfect.
Common Features of Dentinogenesis Imperfecta
all teeth are discoloured (types 2 and 3 more prominent)
bell-shaped crowns
attrition
obliteration of root canals in Type 1 and 2 (more marked in the permanent dentition)
enamel is lost early in Types 1 & 2 due to a defect in the DEJ (no scalloping of the DEJ)
difficult to differentiate Types 1 and 2 clinically and radiographically
Type 1 is always associated with osteogenesis imperfecta while Type 2 is never associated unless by chance
 Frontal view of dentinogenesis imperfecta (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). Frontal view of dentinogenesis imperfecta (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|
|
 PA radiograph of dentinogenesis imperfecta illustrating bell-shaped crown on mandibular first molar (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). PA radiograph of dentinogenesis imperfecta illustrating bell-shaped crown on mandibular first molar (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|
|
Occlusal view of a patient with dentinogenesis imperfecta illustrating the severe attrition of all of the maxillary teeth (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|
|
 BW radiograph of dentinogenesis imperfecta illustrating obliterated pulps (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). BW radiograph of dentinogenesis imperfecta illustrating obliterated pulps (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|
|
 PA radiograph of dentinogenesis imperfecta illustrating shell teeth (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). PA radiograph of dentinogenesis imperfecta illustrating shell teeth (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|
Impacted Teeth
These are teeth that are prevented from erupting by some physical barrier. The aetiology can be due to a lack of space (crowding) or a rotated tooth germ (so that the tooth is 'aimed' in the wrong direction).
Most Common Impacted Teeth
third molars
maxillary canines
premolars
supernumerary teeth
|
|
|
 PA of impacted permanent mandibular right third molar (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). PA of impacted permanent mandibular right third molar (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|
|
 PA of impacted permanent mandibular right canine; the crown is undergoing resorption (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). PA of impacted permanent mandibular right canine; the crown is undergoing resorption (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
|
|
|

Panoramic radiograph of impacted third molars; the maxillary right third molar is both impacted and inverted; both of the mandibular third molars exhibit a 90 degree horizontal rotation (courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|
|
Panoramic radiograph of a patient with multiple impacted and supernumerary teeth (courtesy of Dr. BM Cleghorn, Dalhousie University).
|
|









 Secondary Maxillary Right Central and Lateral Incisors
Secondary Maxillary Right Central and Lateral Incisors
 Radiograph of extracted maxillary third molar with two enamel pearls on the root (courtesy of Dr. BM Cleghorn, Dalhousie University).
Radiograph of extracted maxillary third molar with two enamel pearls on the root (courtesy of Dr. BM Cleghorn, Dalhousie University).



 Periapical radiograph of mandibular molars illustrating a taurodont mandibular left second molar (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba)
Periapical radiograph of mandibular molars illustrating a taurodont mandibular left second molar (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba) Periapical radiograph of mandibular molars illustrating a taurodont mandibular left second molar (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba)
Periapical radiograph of mandibular molars illustrating a taurodont mandibular left second molar (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba) Extracted permanent maxillary left central incisor with a short dilacerated root. This was caused by a traumatic injury at the time when the root was just beginning to form. The primary central incisor had been intruded causing the permanent maxillary incisor to have a stunted, dilacerated root (courtesy of Dr. BM Cleghorn, Dalhousie University).
Extracted permanent maxillary left central incisor with a short dilacerated root. This was caused by a traumatic injury at the time when the root was just beginning to form. The primary central incisor had been intruded causing the permanent maxillary incisor to have a stunted, dilacerated root (courtesy of Dr. BM Cleghorn, Dalhousie University).
 The clinical photo on the left illustrates a permanent maxillary right lateral incisor with a notch in the incisal ridge. This macrodont tooth has a single root canal system and is an example of gemination (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
The clinical photo on the left illustrates a permanent maxillary right lateral incisor with a notch in the incisal ridge. This macrodont tooth has a single root canal system and is an example of gemination (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
 The clinical photo on the left illustrates permanent maxillary right and left central incisors with notches in the incisal ridges. These macrodont teeth both have a single root canal system and are examples of gemination (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
The clinical photo on the left illustrates permanent maxillary right and left central incisors with notches in the incisal ridges. These macrodont teeth both have a single root canal system and are examples of gemination (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). The photo on the left is an example of concrescence between the permanent maxillary right second and third molars (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
The photo on the left is an example of concrescence between the permanent maxillary right second and third molars (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
 The clinical photo on the left illustrates a buccal view of an extracted mandibular third molar with accessory root (courtesy of Dr. BM Cleghorn, Dalhousie University).
The clinical photo on the left illustrates a buccal view of an extracted mandibular third molar with accessory root (courtesy of Dr. BM Cleghorn, Dalhousie University).
 Occlusal view of a maxillary second premolar with dens evaginatus (courtesy of Dr. BM Cleghorn, Dalhousie University).
Occlusal view of a maxillary second premolar with dens evaginatus (courtesy of Dr. BM Cleghorn, Dalhousie University).
 Mulberry molars (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
Mulberry molars (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).



 Generalized fluorosis (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
Generalized fluorosis (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
 PA radiograph of Type 1 dentin dysplasia illustrating short roots, and crescent-shaped pulp chambers (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
PA radiograph of Type 1 dentin dysplasia illustrating short roots, and crescent-shaped pulp chambers (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). PA radiograph of Type 2 dentin dysplasia illustrating pulp stones, normal root length, and "thistle tube-shaped" enlargements of the pulp chambers (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
PA radiograph of Type 2 dentin dysplasia illustrating pulp stones, normal root length, and "thistle tube-shaped" enlargements of the pulp chambers (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). PA radiograph of the mandibular right quadrant illustrating the "ghost-like" appearance of the affected teeth (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
PA radiograph of the mandibular right quadrant illustrating the "ghost-like" appearance of the affected teeth (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba). PA radiograph of the mandibular right quadrant illustrating the "ghost-like" appearance of the affected teeth (courtesy of Dr. John Perry, University of Manitoba).
PA radiograph of the mandibular right quadrant illustrating the "ghost-like" appearance of the affected teeth (courtesy of Dr. John Perry, University of Manitoba). Periapical cemental dysplasia initially presents as periapical radiolucencies in the mandibular incisor region
Periapical cemental dysplasia initially presents as periapical radiolucencies in the mandibular incisor region Periapical cemental dysplasia at a later stage; the apical lesions become radiopaque over time; teeth remain vital (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
Periapical cemental dysplasia at a later stage; the apical lesions become radiopaque over time; teeth remain vital (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
 PA radiograph illustrating hypercementosis in the apical third of both the mesial and distal roots of the permanent mandibular right first molar (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
PA radiograph illustrating hypercementosis in the apical third of both the mesial and distal roots of the permanent mandibular right first molar (courtesy of Drs. Steve Ahing and John Perry, University of Manitoba).
 Extracted mandibular third molar with tetracycline staining on the cervical half of the root (courtesy of Dr. BM Cleghorn, Dalhousie University).
Extracted mandibular third molar with tetracycline staining on the cervical half of the root (courtesy of Dr. BM Cleghorn, Dalhousie University).